
WE ARE ALL DRINKING COST EFFECTIVE INVESTMENTS WHILE BREATHING FALSE ECONOMIES

At the Studio XVI gym in Stockholm, owner Henric von Zweigbergk watches over his clients, safe in the knowledge that he is protecting their health – not through exercise, but by ensuring they have clean air to breath while they grunt and pant on the treadmills and weights. In a scene repeated across a small but growing number of commercial businesses, from coffee shops to care homes, bookshops to supermarkets, Studio XVI gym has installed an air cleaning system that silently and constantly kills pathogens, making the air safe for all to breath.
The ongoing COVID-19 pandemic1 is both bringing home how dangerous shared indoor air can be, while simultaneously showcasing multiple ways to control and eliminate these dangers. It has also demonstrated societies striking inertia to adopt proven technologies that carry clear societal benefits. Each year, airborne viruses such as SARS-CoV-2, other coronaviruses, influenza, RSV and rhinovirus cause billions of instances of illness, and lead to severe infection or death for tens of millions. Tuberculosis, a disease which is solely transmitted through the air still continues to kill 1 million people a year. Yet when you present solutions – clean air technologies – a common rebuttal is ‘it’s too expensive.’ This is an odd response because when applied to water, the financial outlay required to provide safe, disease free water is never questioned, and is accepted as the status quo.
Others have asked why we don’t clean air like we clean water. This short essay invites you to flip this question on it’s head and ask why don’t we manage waterborne threats like we currently manage airborne diseases?
This year Britain invested £15.4 billion in cleaning water, equating to £226 per person. Every day 16 billion litres of water – six and a half thousand Olympic-sized swimming pools – is collected, stored, treated and then transported through 810,000 km of pipes and sewers – a distance sufficient to reach the moon and back.
Water is cleansed of pesticides, pharmaceuticals, nitrates, phosphorous, bacteria, viruses, protoctists and Uncle Tom Cobley and all. This is performed through numerous treatments including filtration, activated carbon treatment, reverse osmosis, oxidation, UV disinfection and chlorination. Water quality is monitored through regular sampling. Collecting, treating and moving water is a complex and costly business.

Sampling water quality in a UK treatment plant
But what if we started to think that, like with air, the £15.4bn was ‘too expensive’ and looked for an alternative strategy? How would that work? We wouldn’t want to regress back to pre-industrial times, so we could make the collection and storage of water an individual responsibility, while tapping into the resources the pharmaceutical industry and modern medicine can provide to tackle the various consequences of untreated water. We could;
– vaccinate everyone periodically for typhoid/cholera (c 60% efficacy – slightly better than the current influenza and COVID-19 vaccines – but still leaving many people unprotected).
– vaccinate against hepatitis A, a virus associated with a lack of safe water and poor sanitation
– massively boost production of antibiotics for parasitic protoctist infections such as giardiasis, cryptosporidium, cyclosporiasis and for bacterial infections such as leptospirosis, campylobacteriosis, legionellosis and dysentery that we don’t have vaccines for.
– increase production of oral hydration treatments for e-coli and salmonella among others
– medication to treat toxic algae bloom poisoning

Parasitic protoctist – giardiasis
We would also need extra NHS resources: more doctors and nurses to cope with increased GP visits; more hospital beds: and additional resources for treating the high-risk groups disproportionately affected by waterborne diseases. We would also need to plan for permanent increases in sick leave, loss of economic productivity and disruption of children’s education.
The impacts would stretch further. Many researchers now believe that cleaning polluted water historically led to a decrease in non-water transmitted contagious diseases such as TB and pneumonia.
“The leading explanation seems to be that contaminated water weakens the immune system, making one susceptible to other contagious diseases, not just typhoid “(Harvard economist David Cutler)
Therefore, if we stopped treating water we should also expect to see a more general rise in sickness and mortality from these secondary undesirable effects.
For those who have the resources, investment in domestic scale water treatment systems would be feasible, but once outside the home, safe water would not be guaranteed in workplaces, public buildings and leisure facilities.
In Britain, if we did apply the same strategy we are using to manage airborne infections to water, abandoning that £15.4 billion annual investment in favour of downstream mitigations, would this be cost effective? I think we can all agree that we would be hard pressed to find any health agency, commercial enterprise, government or voter that would support such an approach. It would be far more costly, socially devastating and economically damaging for any country to switch to such a reactive system. Instead, we all accept a state mandated system, with legal obligations to pay for and provide safe water, within well defined statutory requirements, because we’ve learned from a long history that this is by far the most efficient way to manage water.
Even with clean water, the previously mentioned medical interventions can be vital for civil emergencies (such as floods) rare system failures and for some participating in recreational outdoor water activities, but they are not used on a routine basis. Outside the UK they remain essential for the one billion of people who still lack access to safe piped water, but here the WHO continues to advocate for ‘point-of-use’ strategies for clean water supply, rather than mopping up the mess caused by dirty water.
It’s not as though we don’t have comparable technologies to clean indoor air as well – we do. And, unlike the bulky nature of water that requires huge infrastructure to store and transport from one location to another, indoor air can be treated in-situ. We have companies specialising in particle monitoring systems for real time detection of airborne pathogens. The highly effective UVC/Far-UVC disinfection solutions are available and continuously developing. We have the well established filtration technologies, and the relatively recent CO2 monitoring innovations are now being applied to public indoor spaces.
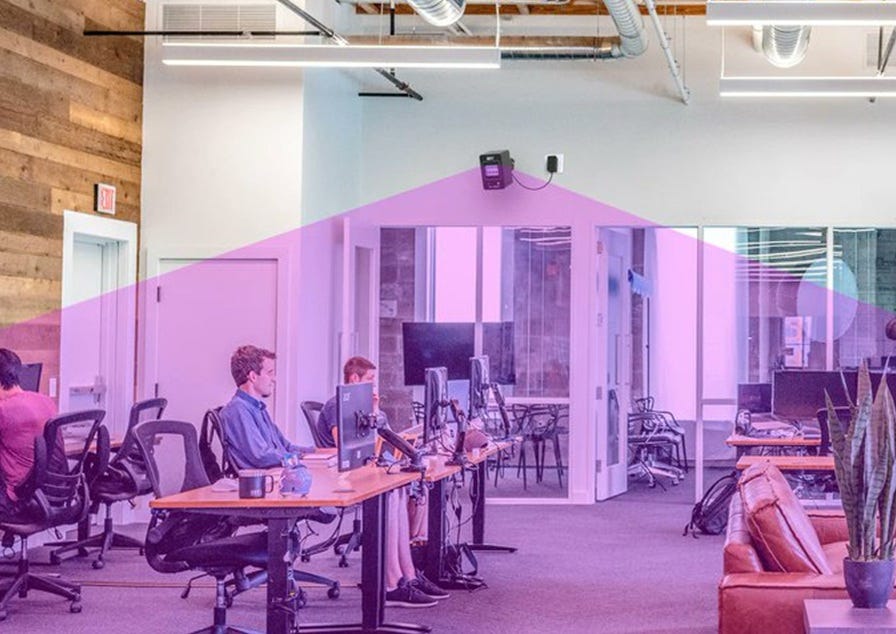
Far-UVC at work in an office space
Governments have yet to appreciate the false economy of their failure to address the issue of shared indoor air, but where clean air technologies in the business world have been fully embraced, we are starting to see some remarkable results. In the US, Sunrise Senior Living care facilities installed comprehensive Far UVC systems across three of their largest facilities. Compared with the previous year they achieved
– 92% reduction in respiratory illnesses – effective elimination
– 78% decrease in antibiotic prescriptions for respiratory conditions – vitally important considering the WHO’ s warning: “Antimicrobial resistance is outpacing advances in modern medicine, threatening the health of families worldwide”
– 65% reduction in resident hospitalisations due to infections
– 43% decrease in staff sick days related to respiratory illnesses
Equally staggering were the economic benefits, with the return on investment achieved in just 9 months. As a result Sunrise Senior Living has approved the rollout of Far UVC systems to all of their facilities over the next 18 months.

Elderly care home residents enjoying breakfast
Also in the US, Pig Hill Farms are now addressing livestock and human health concerns through installation of Far-UVC systems as a critical biosecurity solution, especially in the light of the recent surge in highly pathogenic avian influenza cases. EuroShop, the world’s no.1 retail fair is increasingly seeing businesses investing in modern hygiene technologies to protect both customers and staff from the threat of both airborne and surface pathogens.
“Investments in modern hygiene technology pay off twice over: They not only increase objective cleanliness but can also strengthen the brand image and promote customer loyalty.” Sven Reck (EuroShop)
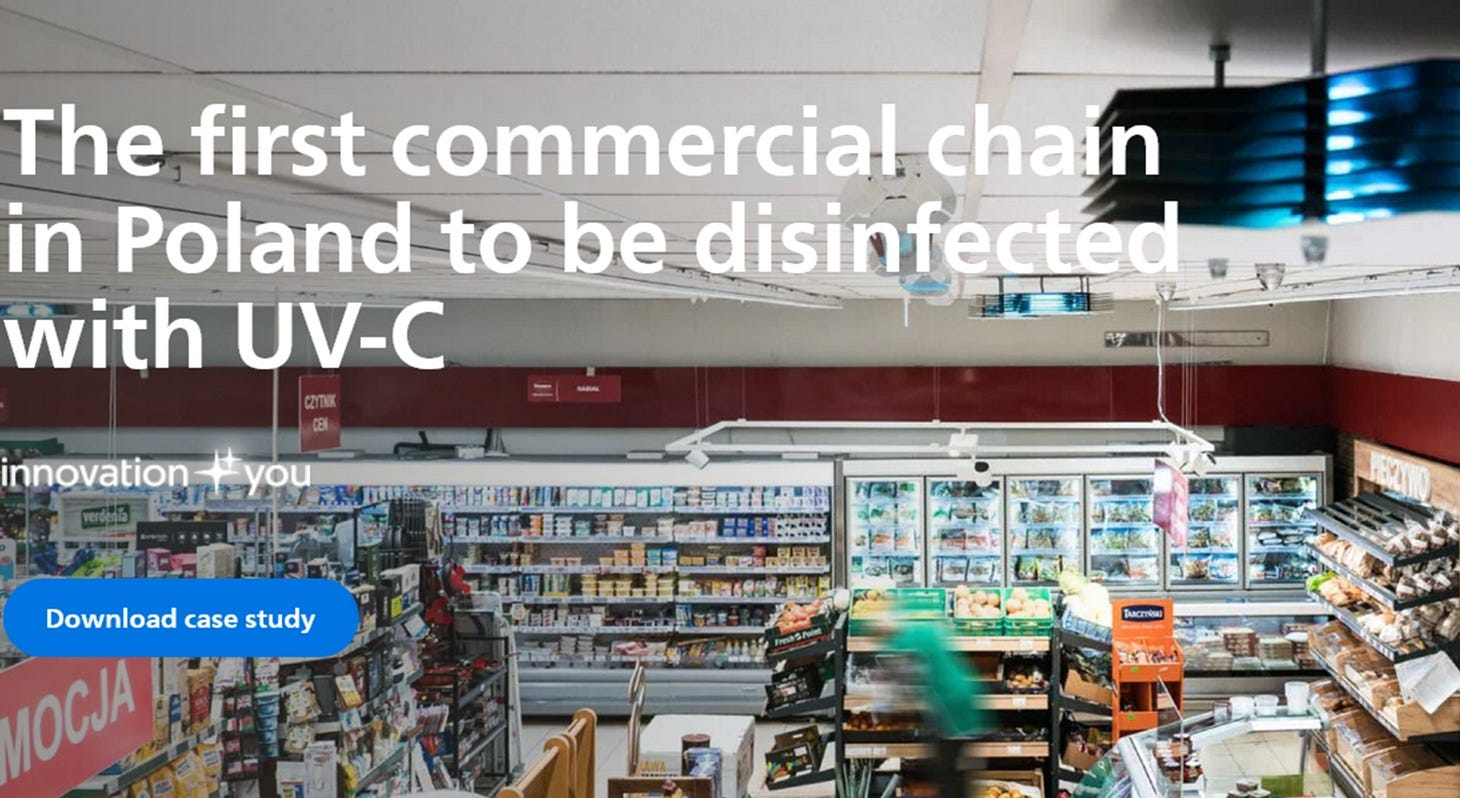
UVC air disinfection in retail setting, from https://www.lighting.philips.co.il/support/cases/food-and-large-retailers/dm-shops
The thread that links all of these disparate businesses is – money. Happy and still alive elderly care home residents bring in more income, gym owners don’t want their customers to be ill in bed with ‘flu or COVID, missing sessions, and healthy pigs are highly profitable. Through investing in clean air technologies they believe they have a competitive advantage – it’s that simple.
I find it strangely perverse, that my prior belief that leftist collective political sentiments and strong societal leadership have not been successful drivers of a compassionate health policy: rather, it increasingly appears that it is the business world that is driving clean air initiatives, precisely because the ‘do nothing’ status quo is the less cost effective option. But compassion is also cost effective – they are not mutually exclusive.
UK government policies around the dangers of shared indoor air are riddled with distorted perspectives. When in opposition, Labour spoke harshly about illegal sewage dumping, which led to 3,286 hospital admissions in 2022-23 from waterborne infections, an increase of 60% since 2010. They said this was “unacceptable”, “sickening”, and placed additional pressure on the NHS, promising they would take tough action. Yet, over the last twelve months, admissions to hospital from a single contagious airborne disease – COVID-19 are approaching 60,000. Despite being 20 times greater than all waterborne admissions combined, Labour is silent.
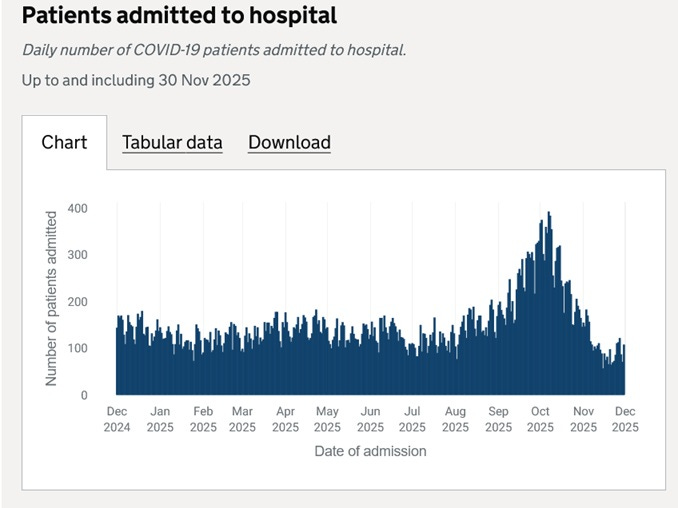
UKHSA COVID-19 Hospital admissions data year to December 2025
North of the border, the Scottish government has announced that there has been a 2.4 million increase in GP consultations over the last 12 months. I’d bet my mortgage that many of the extra 2.4 million visits are a consequence of the pandemic and are preventable. The solution – an extra 171 doctors, and an additional investment of £531 million – is presented as positive news, but is in fact a clear sign of failure. We should be asking – why are we all becoming sicker?
Excluding all other airborne diseases, studies show that COVID alone costs Britain annually £4.2bn in additional NHS care and £10.5bn in lost work capacity/informal care costs. That’s almost the entire annual investment in water treatment frittered away on the impacts of a single airborne disease.
I believe that the key problem is that, unlike water – a commodity supplied by a corporation, company or public authority, acting under state regulation – the shared air we breath is free. No one pays for it, so no one takes responsibility. There is no question that this attitude is costing far more than it would to tackle the issue – just as we all accept with water. I suspect that at some point in the future, state mandated strategies to provide safe indoor air for all, will be seen as the most compassionate and the least expensive option. But only when the penny drops that we are all drinking cost effective investments while breathing false economies.
1Defined as showing periodic exponential growth cutting across international borders.
The water treatment comparison here is kinda brilliant. We spend £226 per person per year on water without questioning it bc everyone accepts clean water as baseline, but airborne pathogen mitigation gets the "too expensive" pushback. That Sunrise Senior Living data with 92% reduction in respiratory ilness is pretty wild tho. If ROI happens in 9 months the math on this seems pretty straightforward.
Thank you so much for this excellent article. I shared it to Bluesky -
https://bsky.app/profile/taniaspencer.bsky.social/post/3m7xpr2qeis2w